
Looking at the history of dental lights tells us a lot about how we arrived at our current viewpoint.
Dental loupes were introduced to supplement visual acuity on top of pretty terrible 1,500 foot candle dental lights. Early loupe lights were not great, and I actually had one with a giant box on the wall and a big heavy cable to feed the light.
As loupe lights got better and less bulky it became reasonable to ask the question of whether we even needed intraoral lights. And, of course, salespeople for expensive loupes were quick to tell prospective customers that loupes provided all of the illumination needed for providing dental care. But loupe salespeople and manufacturers, who aren't dentists, don't understand the nuances of comprehensive dental care or the improved landscape of intraoral lighting.

Dr. David Ahearn, DDS, working with a skilled dental assistant
So how do you know if you need an intraoral light in your dental practice?
Your decision should come down to 4 factors:
- How do you use or intend to utilize assistants?
- How much comprehensive care do you provide?
- How long are your procedures?
- Do you work in the evening or do any sedation work in practice?
Let me simplify this right now as much as possible. You absolutely can use loupes without an intraoral light if:
First, you don’t intend to use Certified Dental Assistants (CDAs) or Expanded Functions Dental Assistants (EFDAs) to the full extent. But, if you use well-trained assistants frequently and often have them cross over to the dental chair, then they either cannot use loupes on the assistant side or need a lower power, higher depth of field loupe set to make this work. You can do it, but there is a specific way to do it right.
Second, if 90% of your work is single tooth, the limited field of view of a higher powered loupe is fine. But if you work cross arch frequently as with paralleling bridge preps or implant placement, you are a great disadvantage in not being able to view the full field extremely well and the best way to do that is with a dental light!
Last, but not least, if you don’t do sedation or anxiolysis and only treat non-anxious patients, the patients that you will be treating are much less affected by the bright room lighting necessary to make loupe-only viewing reasonable.
When you must consider an intraoral dental light
But dental lights must be a consideration for anybody that practices with extraordinary dental assistants, commonly performs larger cases with cross-arch ramifications, or treats anxious patients, perhaps with sedatives.
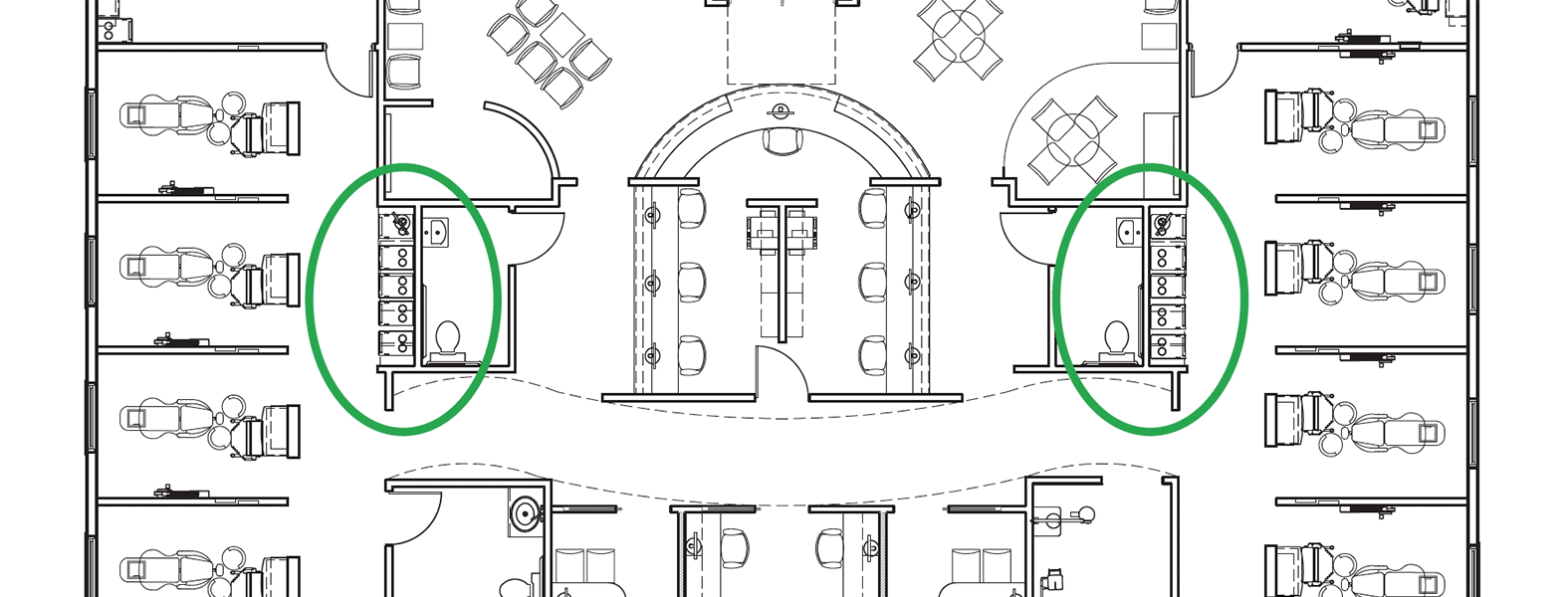
Let’s focus on the doctor assistant interaction first because it’s essential. If your assistant needs to shift from chair side to the operator stool, the focal lengths are 6 to 8 inches different in those two locations. This makes it extremely difficult for an assistant working under loupe lighting to control the entire field. When in the assistant seat, his or her light is not in the right position and the loupe doesn’t have the right focal length.
Now let me clarify. If you were doing all of your treatment on one or two teeth at a time, then the wider field of view that an intraoral light provides is less critical. But most doctors doing bigger cases of any sort involving multiple specialties at once need to rapidly survey the entire field. To be able to illuminate the entire mouth well you need a dental light. Now I know that there’s another school of thought that has told you you can use in-mouth, intra-oral illumination to light up the whole mouth. But here’s why that's a flawed approach. Lighting works well when it is parallel to your field of view, not when it is in opposition or perpendicular. Staring at lightbulbs while successfully illuminating an area is a horrible way to go ahead and gain visual acuity. There are some companies that yell at me a lot about the statement, but this is simply the laws of physics.
Remember, I am a huge loupe proponent when they are carefully used in a specific way. When you don’t do this, you’ll wind up with loupes that increase problems with your ailing back, you’ll have an assistant team that can’t grow to their potential, and you’ll wind up with no more productivity than you had before you got the new high powered loupes.
So why doesn’t everybody love intraoral lights?
The essential issue with intraoral lights is that most of them, quite frankly, are poorly designed and manufactured. Pole mount lights bounce with the chair, drift, and are pretty hideous aesthetically if you’re trying to make your practice look non-clinical. Point ceiling mount lights get stuck in odd rotational positions and tend to be a hassle to move around. Wall or cabinet mount light have long arms that tend to drift. And traditional track lights get out of adjustment and have sticky cables that wear out in their tracks.
Frustrated with these options, I decided over a decade ago that I would develop the perfect room light systems to improve patient comfort and to reduce operator eyestrain. I knew that pole, point ceiling, and wall or cabinet mount lights were not viable options. This left track lights, which at the time, had their own issues. They were:
- Too expensive
- Too hard to install
- Prone to getting out of adjustment
- A total … bugger … to service
Creating the best dental track light systems
Targeting track lights as the best option for dental lighting, my team went out and fixed all of the issues that have hampered tracks forever. What did we do with our Aurora and FastTrack Lighting Systems?

The Aurora Lighting System provides spot, intraoral, and beautiful diffuse full-room lighting along with patient media
First, when you cast the chassis in one piece instead of screwing a bunch of cheap scraps together, it can’t get out of adjustment.
Second, if you create a patented system to mount them you can even install the thing yourself. One person. It’s that easy.
Third, when you create raceway tracks inside the solid chassis you can utilize industrial chain carriers to manage the cabling. They are proven to run at least 50 years worth of cycles in a dental setting.

Details matter. Aluminum chassis and chain carriers to manage the cabling in the FastTrack Lighting System.
And last, if you eliminate the middleman, even with the much more expensive design, cost still comes down. So do you need a dental light? I’m thinking that if one good crown and bridge case pays for all of the lights you’ll need, that the answer is probably yes.
For more inspiration, take a look at our recent dental office design work. If you have any questions, please reach out to my team at Design Ergonomics.
You may also be interested in:

The Math of Dental Practice Growth
The average concept-to-completion time-frame for construction is nine to twelve months. By the time you need to bring on an associate with two-to-three rooms of their own, if you haven’t started planning for it, you’re already a year behind.
Read more
Topics:





















{kind=link}